

Wilson's disease is a familial, chronic and life-threatening copper metabolism disorder that requires urgent medical evaluation and treatment.
What physiological role does copper play in the body?
Copper is essential as a trace element because it is involved in essential metabolic processes in various organs and tissues.
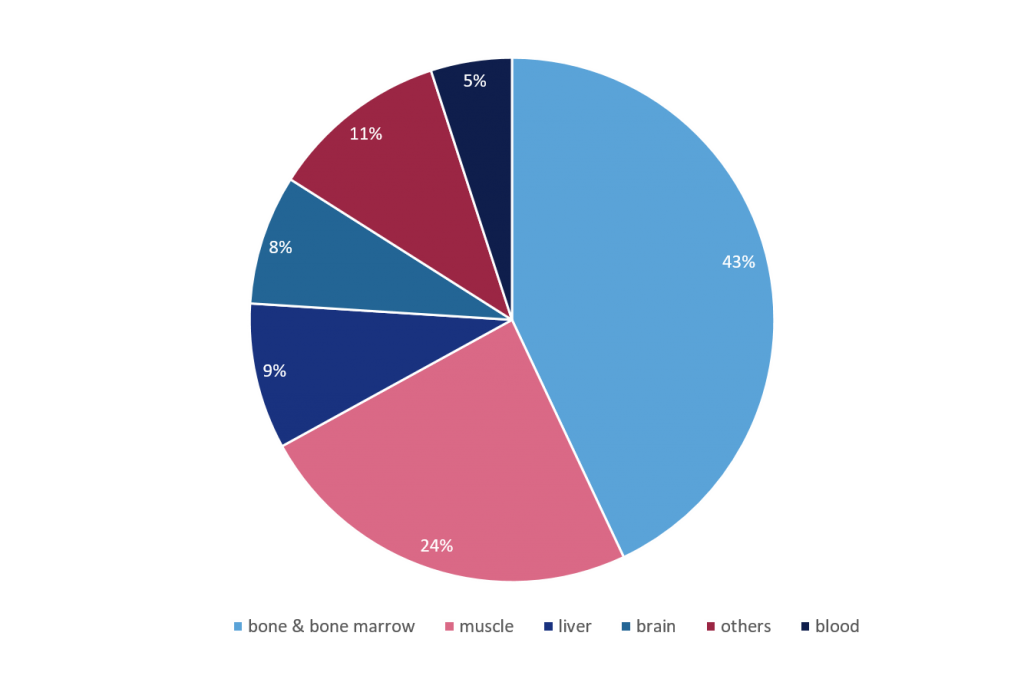
The percentage distribution of copper in individual organs and tissues of the human body is estimated as follows:
Examples of endogenous processes in which copper plays a role:
Under normal circumstances, the amount of copper is highly regulated, as non-protein-bound copper reacts toxically in the body and leads to severe organ damage at high concentrations. Therefore, the German Nutrition Society recommends the following estimated values for an adequate daily intake:
| Infants 0 - 4 months | Infants 4 - under 12 months | Childs 1 to 7 years | Childs from 7 years old to adults | |
| Copper mg/day | 0,2 - 0,6 | 0,6 - 0,7 | 0,5 - 1.0 | 1,0 - 1,5 |
For example, 1 mg copper is contained in:
| Food | Quantity (in grams) |
|---|---|
| Nuts | 25 |
| Cocoa powder | 25 |
| Brewer's yeast | 25 |
| Liver | 25-50 |
| Mussels | 40 |
| Oysters | 50 |
| Chocolate | 50 |
| Wheat germ | 50 |
| Wheat bran | 60 |
| Legumes | 100 |
| Wholemeal rye flour | 125 |
| Cheese | 100-500 |
Although it is primarily the liver and brain that are restricted in their function, other organs can also be affected. According to epidemiological studies, the first symptoms appear between the ages of five and 45, and rarely thereafter.
Symptoms include:

Hepatic: chronic. hepatitis, liver cirrhosis and even liver failure. Symptoms usually appear from the age of 2.

Neurological: motor and coordination disorders can occur occasionally, such as tremor, movement disorders, but also writing, swallowing and speech disorders. Symptoms usually appear from the age of 15.

Psychiatric: psychiatric changes such as concentration disorders, mood swings or depression appear in about one third of those affected. Symptoms usually appear from the age of 15.
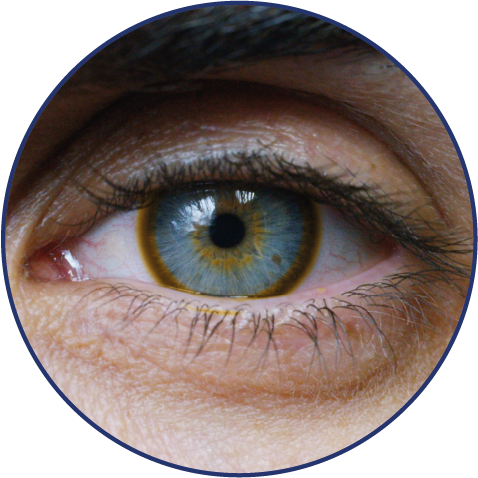
Ophthalmological: about 80% of patients show so-called Kayser-Fleischer rings, which stand out due to a 1-3 mm wide greenish-brown, reddish or golden-brown ring at the edge of the cornea. The rings are caused by copper deposition and do not have to be completely closed. The symptoms usually appear from the age of 10.
The course of Wilson's disease sometimes varies greatly from patient to patient. This depends, among others, on the following factors:
If the diagnosis is made relatively early, i.e. in the still asymptomatic stage, and if therapy is initiated early and maintained throughout life, those affected have a fundamentally positive prognosis with regard to their life expectancy.
The presumption of Wilson's disease usually follows:
The diagnosis is then usually confirmed by a number of tests. The following measures, among others, are taken to clarify the findings:
Although there is currently no cure for Wilson's disease, several oral medications are available that:
Drug therapy is basically divided into two mechanisms of action:
| Remove accumulated copper from the organism | Preventing a renewed copper uptake |
| To remove the excess copper from the tissues and organs, copper chelators are mainly used. The excess copper is then excreted from the body through the urine. | Another possibility is the use of preparations containing zinc, for example; these are intended to prevent the gastrointestinal tract from absorbing copper from food. In this way, a new accumulation can be prevented. |
Furthermore, in addition to a mandatory lifelong medication, a low-copper diet is advantageous. Supplementation with antioxidants such as vitamin E could also support the therapy of Wilson's disease.
In severe cases with a fulminant course, a liver transplant may be necessary for survival.
The information on this website is for general educational purposes only and is not intended to make a diagnosis or to recommend a treatment. Please consult a doctor for any medical questions regarding this condition.
Członkowska A. et al. Wilson disease. Nat Rev Dis Primers 2018; 4: 21. 2. Wilson’s Disease Association www.wilsonsdisease.org (download: Juni 2020)
EASL Clinical Practice Guidelines (2012). Wilson’s disease, Journal of Hepatology 2012; 56: 671-685. www.easl.eu (download: Oktober 2021)
Ferenci, P. et al. Age and Sex but Not ATP7B Genotype Effectively Influence the Clinical Phenotype of Wilson Disease. Hepatology 2019; 69: 1464-1476. https://doi.org/10.1002/hep.30280
https://www.deutsche-apotheker-zeitung.de/daz-az/2007/daz-49-2007/basiswissen-ernaehrung-folge-20 (download: 28.10.2021)
https://www.dge.de/wissenschaft/referenzwerte/kupfer-mangan-chrom-molybdaen/ (Abruf: 18.10.2021)
https://dgn.org/leitlinien/ll-14-2012-morbus-wilson/ (download: 18.10.2021)
Marktl W. Physiologie und Ernährungsphysiologie von Kupfer. Journal für Mineralstoffwechsel & Muskuloskelettale Erkrankungen. 2000; 7(2): 27-30
Hermann W. und Huster D.Diagnostik des Morbus Wilson. Nervenarzt 2018; 89: 115–123
Wilson's Disease Tool - ESPGHAN (Download 22.10.2021)